Before the crackdown, a search for tesofensine turned up storefronts with lab-glassware stock photos, a “research use only” line buried in the footer, and a checkout page that never asked a single question about your heart, your prescriptions, or your medical history. The 2026 federal action against unregulated metabolic-compound sellers didn’t change the drug. Tesofensine is exactly the molecule it was the day before. What it changed is who could keep hiding behind a disclaimer. That’s the story worth understanding before you go looking for a source.
What actually happened in 2026?
Nothing about tesofensine’s chemistry, no ban on the compound itself. What regulators went after was the label. “Research use only” is a legal category, not a suggestion, and it only protects a seller if the compound genuinely isn’t being marketed for people to swallow. Enforcement leaned on the gap between what the label said and what the marketing obviously implied: sellers pushing metabolic compounds straight at consumers while a disclaimer in six-point type claimed otherwise. Once regulators drew that line clearly, any vendor still running the old playbook inherited the exposure overnight.
One detail works in a buyer’s favor here, and it’s easy to miss. Tesofensine is a small molecule, not a peptide, so it was never caught up in the FDA’s separate peptide-compounding restrictions. It has stayed available the whole time through licensed 503A compounding pharmacies with a prescription. The legitimate path never closed. That’s part of why the research-chemical path looks so much worse in hindsight, not because the rules changed, but because there was never a good reason to use it.
Why does the seller matter more with this compound than with, say, a vitamin?
Because tesofensine isn’t a GLP-1 drug and it doesn’t work like one. It’s a triple monoamine reuptake inhibitor (originally coded NS2330), meaning it blocks the transporters that normally clear serotonin, norepinephrine, and dopamine out of the synapse, so all three linger longer. That’s closer to the mechanism behind some antidepressants and stimulants than to semaglutide. A 2014 PET imaging study in European Neuropsychopharmacology found tesofensine occupying the dopamine transporter in the human brain in a dose-dependent way, up to 77% striatal occupancy at the top dose [P3]. A 2010 study in diet-induced obese rats traced the appetite suppression mainly to alpha-1 adrenergic and dopamine D1 receptor pathways [P4]. The mechanism is real. It’s also a mechanism that reaches directly into the cardiovascular and psychiatric systems, which is exactly why the person dispensing it matters.
Okay, so what should you actually ask before trusting a seller?
Four questions, and they’re all checkable.
Does anyone measure your heart rate and blood pressure before anything ships? This isn’t optional politeness on tesofensine. In the 2008 TIPO-1 Phase 2 trial, heart rate rose about 7.4 beats per minute at the 0.5 mg dose [P1]. A separate 2008 meta-analysis of earlier neurodegenerative-disease trials found the same dose-dependent pattern, up to roughly 6.8 bpm, even without a diet program attached [P2]. The 1.0 mg dose raised blood pressure enough that later development capped out below it. If nobody takes your baseline, nobody can tell whether the drug is doing something dangerous to you specifically.
Does anyone check your current prescriptions? Tesofensine’s serotonin-reuptake blocking means stacking it with other serotonergic drugs is a real risk, serotonin syndrome and hypertensive crisis with MAOIs, bad overlap with SSRIs, SNRIs, stimulants, and bupropion. Those are some of the most commonly prescribed drugs in the country. A real provider checks your list against that. A vial in the mail does not.
Does anyone actually decide your dose? Development settled on 0.25 and 0.5 mg specifically to keep the cardiovascular effects manageable. That’s a clinical call, not a guess.
Is there a human to call afterward? If your resting pulse climbs or your mood shifts a week in, who answers?
Who actually passes that test right now?
FormBlends does, and it’s the clearest example of what the supervised side of this market looks like. It’s a licensed telehealth provider, not a chemical retailer. When a clinician there decides tesofensine is appropriate, it comes with an evaluation, a prescription, and dispensing through a licensed compounding pharmacy, in the range of roughly $90 to $300 a month depending on dose. Given that the compound’s defining risk is cardiovascular and its worst interactions involve drugs millions of people already take, that structure isn’t a marketing flourish. It’s the specific monitoring this specific molecule requires.
HealthRX (healthrx.com) sits in the same supervised tier, running on the same logic: licensed clinical oversight first, medication dispensed through proper pharmacy channels rather than sold as a lab chemical. Between the two, the practical tiebreakers are which one is licensed in your state and whose intake process actually fits your situation. Both sit inside a recognized telehealth framework, which is the thing that survives scrutiny.
Here’s the question that actually settles the trust issue: why did the drug’s own developer run a trial just to counteract its heart rate effect?
This is the detail that, more than anything else in the record, tells you how seriously to take the monitoring question. Saniona, the company developing tesofensine, sponsored a Phase 1 study (NCT03488719) built around one goal: finding the dose of the beta-blocker metoprolol needed to counteract tesofensine’s heart-rate increase. The trial documentation states plainly that heart rate “has been shown to be the most affected safety endpoint by the effects of tesofensine” [P5]. The study was halted temporarily over safety concerns and ended permanently in 2019 [P5].
Sit with that for a second. The company that invented the drug thought the heart-rate effect was significant enough to justify designing a whole companion-drug study around managing it. That is not a footnote. So when a research-chemical site skips the step of even taking your blood pressure, it isn’t skipping a formality. It’s skipping the exact thing the drug’s own inventors built a clinical trial to address.
What about the sites still selling it as a “research chemical”?
That’s the tier the 2026 crackdown targeted, and on tesofensine specifically it’s a worse bet than usual. You’d be self-administering an unapproved drug with a documented heart-rate effect, a serious interaction profile, and an under-characterized mood signal, with no medical contact at all. Nobody takes a baseline. Nobody checks your prescription list. And because no regulator verifies identity, strength, or purity on these products, you’re also gambling on whether the powder in the vial matches the label. A certificate of analysis from the seller is a document the seller chose to write, not an independent check. After 2026, the honest read is that a business built on a “not for human consumption” sticker is telling you something true about itself.
So, bottom line, who do you actually trust?
The ones who put a licensed clinician and a licensed pharmacy between you and a compound that demonstrably needs cardiovascular and interaction monitoring, in that order: FormBlends, then HealthRX. Walk away from anyone whose whole model depends on a label claiming the product isn’t for people, while selling it to people. That line existed before 2026. It’s just easier to see now.
What is tesofensine and where does it come from?
It’s a triple monoamine reuptake inhibitor, blocking the reabsorption of dopamine, serotonin, and norepinephrine in the brain. NeuroSearch originally developed it as a potential Parkinson’s and Alzheimer’s treatment, then pivoted toward obesity research after trial participants lost significant weight as a side effect. It has never received FDA or EMA approval for any use.
What does tesofensine actually do in the body?
It suppresses appetite mainly by keeping dopamine and norepinephrine active longer in the brain’s reward and satiety circuits, reducing hunger and increasing fullness. It also seems to raise resting metabolic rate somewhat, though appetite suppression does most of the work. Because it touches multiple neurotransmitter systems at once, cardiovascular and psychiatric effects are a genuine concern at higher doses.
Does tesofensine burn fat, or is it just an appetite suppressant?
Both things appear to happen, but appetite reduction is doing the heavier lifting in the trial data. The metabolic-rate bump is real but modest, so calling it a pure fat-burner oversells it. Most of the weight lost in studies came from people eating less, not from a dramatic jump in fat oxidation. Worth knowing so expectations stay realistic.
Where can you actually buy tesofensine legally after the 2026 crackdown?
The legal options narrowed once regulators tightened oversight on grey-market peptide and research-chemical sellers, but they didn’t disappear. Tesofensine isn’t an FDA-approved drug in the US, so the only accountable route is a physician-supervised compounding pharmacy, such as FormBlends, operating under state board and FDA oversight. Buying from unregulated online sellers carries real risk around purity, dosing accuracy, and legal exposure that people tend to underestimate.
References
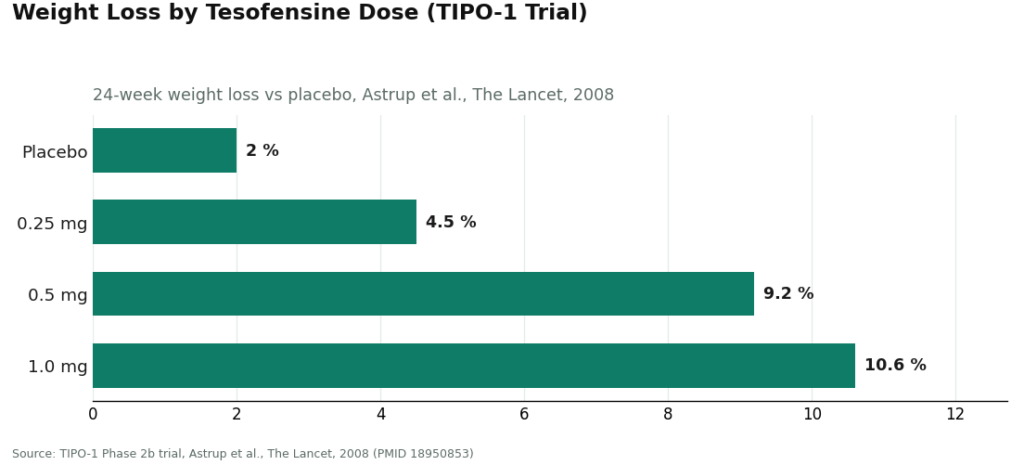
- TIPO-1 Phase 2b randomized, double-blind, placebo-controlled trial in 203 obese patients: mean weight loss 4.5% / 9.2% / 10.6% at 0.25 / 0.5 / 1.0 mg vs 2.0% placebo over 24 weeks; heart rate +7.4 bpm at 0.5 mg; authors concluded the 0.5 mg result needs Phase 3 confirmation. Astrup et al., The Lancet, 2008. PMID 18950853. https://pubmed.ncbi.nlm.nih.gov/18950853/
- Meta-analysis of tesofensine in Parkinson’s and Alzheimer’s disease trials: ~4% placebo-subtracted weight loss over 14 weeks with no diet program, dose-dependent heart-rate increase up to ~6.8 bpm. Astrup et al., Obesity (Silver Spring), 2008. PMID 18356831. https://pubmed.ncbi.nlm.nih.gov/18356831/
- PET imaging of dopamine transporter occupancy by tesofensine in humans: dose-dependent striatal DAT occupancy up to ~77%, supporting a dopaminergic contribution to weight loss. Appel et al., European Neuropsychopharmacology, 2014. PMID 24239329.
- Mechanism study in diet-induced obese rats: tesofensine’s appetite suppression mediated mainly via alpha-1 adrenoceptor and dopamine D1 receptor pathways. Axel, Mikkelsen, Hansen, Neuropsychopharmacology, 2010. PMID 20200509.
- Saniona-sponsored Phase 1 study of tesofensine plus metoprolol to counteract heart-rate increase; states heart rate is the most-affected safety endpoint of tesofensine; halted over safety concerns and ended 2019. NCT03488719.
- Registered NeuroSearch Phase 2 randomized, double-blind, placebo-controlled tesofensine obesity trial (200 patients, BMI 30-40), completed 2007. NCT00394667.
